|
Abstract: |
Epidemiology
Breast cancer is the leading cause of cancer-related deaths in women living in the western world [1]. The crude incidence of breast cancer in the EU is 109.8/100,000, and the mortality is 38.4/100,000 women/year [1]. In industrialised countries in recent years, mortality rates have decreased due to the widespread use of screening programmes and of adjuvant systemic treatment. Because of its high incidence and improving survival, breast cancer is currently the most prevalent cancer in western industrialised countries [2]. With the onset of routine use of screening mammography the anatomic extent of the disease has decreased, with an increase in localised (node-negative) disease. The number of patients with distant disease at diagnosis (~ 5–10%) has not changed and likely reflects a biologically aggressive type of breast cancer that is not affected by early detection [3].
Risk factors
The majority of breast cancer risk factors described in the literature are related to a woman’s lifetime exposure to oestrogens: early menarche and late menopause, a high total number of menstrual cycles, nulliparity and use of dual-hormone contraceptives [4]. Lactation protects against breast cancer while alcohol increases the risk [5]. Breast cancer risk is positively associated with increased smoking during the period between menarche and first childbirth, suggesting that the sensitivity of the female breast to tobacco carcinogens is increased during adolescence and early adulthood [6]. The risk is considerably higher for women with pre-existing risk factors such as older age, a strong family history of breast cancer, a known mutation in the breast cancer predisposition genes, a personal history of therapeutic thoracic radiation, and proven precursor lesions such as atypical ductal hyperplasia.
Diagnosis, pathology and staging
Once a suspicious abnormality is detected in the breast by physical examination or imaging, a definitive diagnosis must be made, with the gold standard being histopathological examination of a biopsy specimen (core-needle or incisional biopsy). Determining the disease stage and detailed pathologic features are important factors for assessing prognosis and choosing the most appropriate treatment for patients with breast cancer.
Most invasive breast cancers are ductal, a combination of ductal and lobular or pure lobular histology. The prognosis of ductal and lobular cancers is similar even though their sensitivity to specific types of treatment differs. Several less common types have more favourable prognoses, such as pure tubular, mucinous or colloid, and papillary cancers. Typical medullary breast cancer is also considered to have a better prognosis, while atypical medullary breast cancers have a prognosis similar to ductal and lobular breast cancers. Metaplastic breast cancer, a relatively rare histological type, has aggressive characteristics and is associated with a poor prognosis. Non-invasive breast cancer or ductal carcinoma in situ (DCIS) do not require adjuvant systemic treatment, although adjuvant tamoxifen may be offered to those with oestrogen receptor-positive to reduce the risk of a second primary breast cancer.
Pathological examination concerns several pathologic features of the tumour, such as size, number of removed and invaded lymph nodes, histological type, nuclear and/or histological grade, proliferation measures, oestrogen receptor (ER), progesterone receptor (PgR) and HER2/neu receptor expression by immunohistochemistry (IHC) or fluorescent in situ hybridisation (FISH)/chromogenic in situ hybridisation (CISH) test.
Staging refers to the grouping of patients according to the extent of their disease and can be based on either clinical or pathologic findings. Tools used to determine disease stage include a physical examination, biopsy, imaging and blood tests. Tumour-node-metastases staging refers to the primary tumour, involvement of the regional lymph nodes and presence of distant metastases.
Standard of care
Treatment for early disease always involves surgery to remove the primary tumour and the affected lymph nodes. Surgical treatment of the primary tumour may occur either by mastectomy or lumpectomy with axillary lymph node dissection or sentinel lymph node (SLN) resection. SLN resection is the preferred method of assessing the pathologic status of the axillary lymph nodes in patients with stage I or II breast cancer. Whole-breast irradiation is recommended for all patients undergoing breast-conserving surgery, whereas radiation of the chest wall and regional lymph nodes is suggested following mastectomy in selected high-risk patients. Adjuvant systemic therapy (chemotherapy and/or hormonal therapy) is indicated based upon risk of recurrence (estimated-based upon morphological (tumour size, grade, lymph node status) and molecular (hormone and human epidermal growth factor receptors 2 (HER2), proliferation) features of the primary tumour and on some patient characteristics (age, menopause status) counterbalanced by co-morbidities and risk of severe side effects and always taking into account the patient’s preferences.
The aim of medical treatment for early breast cancer is to eradicate micrometastases, avoiding relapse and trying to cure the patient. About 30–50% of breast cancer patients develop local or distant relapses after curative surgery. Unfortunately, after clinically evident metastases have been established, the disease is largely incurable.
Treatment decisions should be made by a multidisciplinary team involving among others, medical oncologists, breast surgeons, radiation oncologists, radiologists, pathologists, and psychologists. Since metastatic breast cancer is virtually incurable, there has been a tendency to over-treat patients with early disease, particularly in terms of adjuvant chemotherapy. In recent years, intensive efforts have been made to identify tools to improve prognostication. Examples are the Nottingham Prognostic Index [7], the St Gallen’s risk categories [8] and computer-based algorithms such as Adjuvant! Online [9] that incorporates some clinico-pathological features.
More recently, tools that incorporate biological characteristics of the tumour have been developed using a new technology called gene expression profiling. During gene expression, the mRNA molecule is translated within the ribosome to produce a complete protein and, therefore, counting mRNA transcripts provides an estimate of the number of corresponding proteins. High-throughput technologies, such as DNA microarray and real-time reverse transcriptase polymerase chain reaction (RT-PCR), allow simultaneous counting of many gene transcriptions (up to tens of thousands). Using the microarray technology, van’t Veer et al. identified 70 genes expressed differentially between two groups of patients with very different survival outcomes [10, 11].
The authors concluded that the 70-gene signature (MammaPrint) could outperform current clinical risk classifications and therefore could significantly impact on breast cancer management by sparing some women from overtreatment and the unnecessary toxicity of adjuvant chemotherapy. Similarly, Paik et al. have developed a recurrence score (RS) based on 21 genes, which appears to predict the likelihood of distant recurrence in tamoxifen-treated patients with node-negative, ER-positive breast cancer [12, 13]. A final panel of 16 cancer-related genes and five reference genes forms the basis of the RS commercialised under the name of Oncotype DX assay. Both MammaPrint and Oncotype DX have been submitted to several validation studies but their true clinical utility is currently being evaluated in two large, prospective clinical trials: the MINDACT trial (Microarray In Node-negative and 1 to 3 positive lymph node Disease may Avoid ChemoTherapy) for MammaPrint [14, 15] and the TAILORx study (Trial Assigning IndividuaLized Options for Treatment (Rx)) for Oncotype DX [16]. These trials have recently finished accrual and, if their hypotheses are confirmed, the use of these new genomic tools will allow for a better identification of early breast cancer patients who are at enough low risk of relapse to safely avoid adjuvant chemotherapy, and will hopefully provide the definite answer regarding these types of tool.
Gene expression profiling studies have also demonstrated what has long been observed in clinical practice: that breast cancer is an heterogeneous disease with at least four distinct molecular subtypes identified to date: Luminal A and B (which are usually hormone receptor-positive), HER2 positive, and basal-like subtype (characterised by the absence of expression of both hormone receptors and HER2) [10, 12, 17, 18]. Molecular subtyping is not yet available for clinical practice, but may play a role in more sophisticated treatment decision making in the near future.
Because their expression may also predict a benefit from specific therapies, some prognostic factors can also serve as predictive factors, see Table 1.
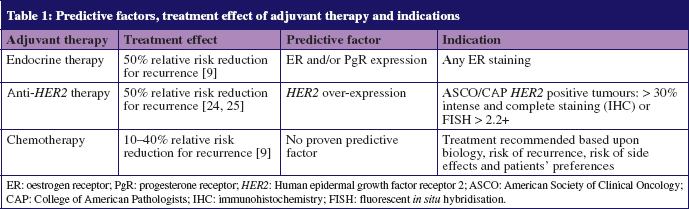
Established predictive factors include ER and PgR expression for endocrine therapy, and HER2 expression for anti-HER2 therapies such as trastuzumab and lapatinib. There are currently no proven biomarkers for response to specific types of chemotherapy. However, several markers seem to indicate a higher likelihood of response to chemotherapy in general, such as an absence of hormonal receptors, high grade and high proliferation measured by Ki67 [19] or genomic tools such as the 70-gene profile [18], the RS [13] or genomic grading [20].
Systemic treatment
Systemic treatment includes chemotherapy, endocrine, and targeted therapy. Therapy may be administered as neoadjuvant treatment, before surgery, or as adjuvant treatment, after curative surgery. The neoadjuvant setting has some advantages, such as shrinkage of the tumour allowing for the resection of otherwise inoperable tumours or breast conserving surgery where mastectomy would be necessary otherwise and in vivo observation of drug effectiveness, but also some disadvantages such as the loss of an accurate axillary staging.
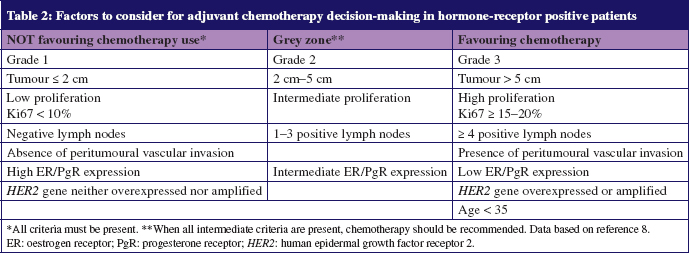
Treatment choice is based on the tumour biology, the patient-risk stratification and the patient’s preferences as outlined in Table 2 [1, 8].
Adjuvant chemotherapy
Ideally, specific adjuvant therapy recommendations should be tailored to the biology of the individual tumour. Low or absent oestrogen receptor levels, HER2 over-expression and increased proliferation (high grade of tumour, high number of mitoses, high Ki67) predict the response to chemotherapy in general, rather than to a specific cytotoxic agent [8].
Evidence from multiple clinical studies indicates that adjuvant chemotherapy in early breast cancer substantially reduces the risk of recurrence. Anthracyclines and taxanes are the most active agents in breast cancer treatment and therefore represent the cornerstones of modern chemotherapy strategies. Anthracyclines have been used in the adjuvant treatment of early breast cancer for more than 25 years. The meta-analysis of randomised trials by the Early Breast Cancer Trialists’ Collaborative Group showed conclusively that anthracycline-based regimens are superior to first generation, non-anthracycline-containing regimens, such as cyclophosphamide, methotrexate, and fluorouracil (CMF) [21]. Treatment with up to six months of anthracycline-based polychemotherapy such as cyclophosphamide, fluorouracil and doxorubicin or epirubicin (FAC or FEC) reduced the annual breast cancer death rate by approximately 38% (± 5%) for women younger than 50 years of age, and by approximately 20% (± 4%) for women aged 50–69 years. However, anthracycline administration is associated with a small (~ 1% but dose-dependent) long-term risk of irreversible cardiotoxicity which manifests clinically as congestive heart failure, and with a very small (~ 0.5%) risk of acute myelogenous leukaemia. This risk must be carefully weighed against the potential benefits of therapy when making individualised chemotherapy recommendations.
Multiple trials have now also demonstrated that taxanes (paclitaxel and docetaxel), whether given concurrently or sequentially following anthracycline-based therapy, provide a further reduction in the risk of recurrence [22]. Since neither group of drugs is effective in more than a minority of breast cancers, their mechanisms of action are different and there is no cross-resistance [23]. Regimens associating anthracyclines and taxanes are preferred, particularly for node-positive disease. These two classes of drugs can be given in combination or sequentially, with recent studies showing an advantage of the sequential strategy. Studies have also shown that the optimal paclitaxel administration is weekly, whereas for docetaxel the optimal regimen is thrice weekly [24].
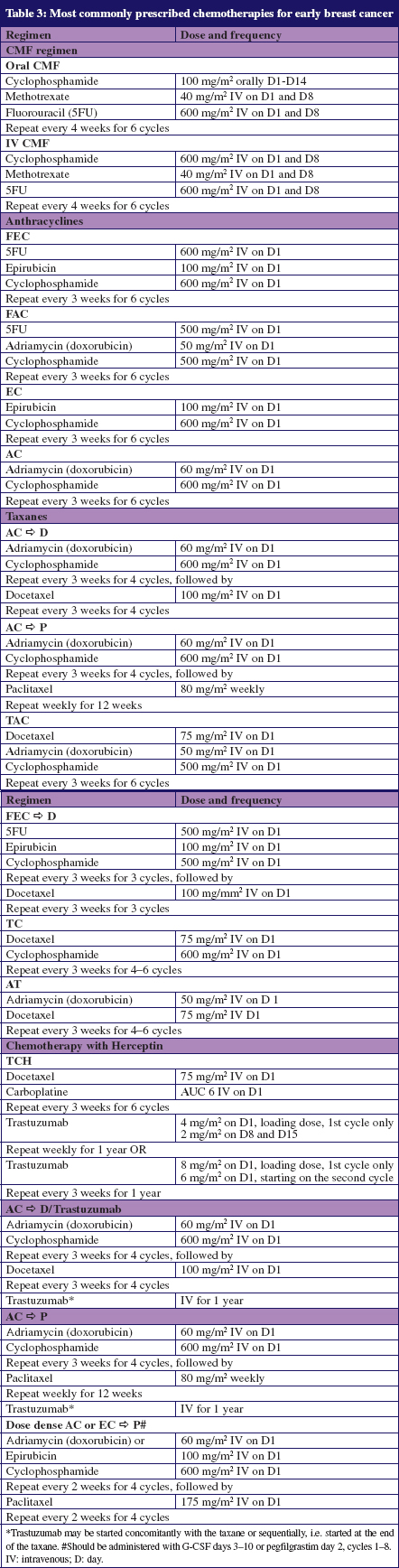
Risk reductions for polychemotherapy are proportionally the same in patients with node-negative and node-positive disease. The benefit of adjuvant chemotherapy must be weighed against potential short-term acute toxicities such as partial or total alopecia, nausea, vomiting, oral mucositis, diarrhoea, constipation, peripheral neuropathy, myelosuppression (neutropenia, thrombocytopenia and anaemia) and long-term toxicities: infertility, premature menopause, cardiomyopathy, acute leukaemia, and neuropathy [25]. Neutropenia is potentially serious because it can lead to infectious complications and death. Granulocyte colony-stimulating factor (G-CSF) can be given as primary prophylaxis, e.g. as a support to dose-dense adjuvant regimens to prevent infectious complications and dose delays, or secondary prophylaxis for those patients who experienced a febrile neutropenia in previous cycles. Long-term serious side effects are rare but include cardiotoxicity with anthracyclines and trastuzumab and a slight increase in the incidence of myelodysplastic syndromes and acute leukaemias particularly with cyclophosphamide. Chemotherapy-related cardiac toxicity from anthracyclines is dose-related and can be irreversible, while cardiac toxicity from trastuzumab is not dose-related, and is largely reversible. The most common chemotherapy regimens used in the adjuvant setting are listed in Table 3.
Adjuvant endocrine therapy
Endocrine therapy for breast cancer has been used for more than a century. Oestrogen deprivation is a key therapeutic approach in the treatment of hormone-sensitive breast cancer. Historically, ablation of endocrine sources such as ovaries, adrenal glands or hypophysis, was effectively used in advanced disease to obtain tumour regression and control symptoms. The use of endocrine treatment for breast cancer has increased due to the development of relatively well-tolerated oral drugs.
Approximately three-quarters of all invasive cancers are hormone receptor-positive. All patients with hormone receptor-positive tumours should be considered for adjuvant endocrine therapy lasting for at least five years, unless clinically contraindicated.
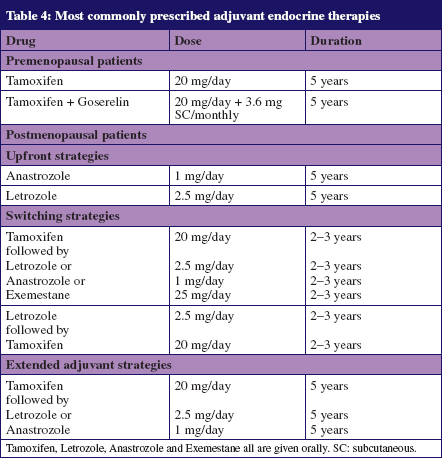
For premenopausal patients, tamoxifen alone (20 mg daily for five years) or the combination of ovarian function suppression/ablation with tamoxifen is the standard of care. Tamoxifen is a selective oestrogen receptor modulator with a long half-life, ranging from 7–14 days, which allows for once daily administration. It has both partial oestrogen agonist and antagonist effects; that is, it antagonises the action of oestrogen in the breast, but mimics oestrogen in other tissues, such as the bone and uterus. Partial agonist effects can be beneficial, since tamoxifen helps to prevent bone demineralisation, increases bone density, and also improves lipid profile [26]. However, the agonistic action also increases the risk of uterine cancer by 2.4 times and the risk of a thromboembolic event by 1.9 times [27]. In ER-positive disease, using tamoxifen for five years reduces the annual breast cancer death rate by 31%, irrespective of age, chemotherapy, and other tumour characteristics [21]. Endocrine strategies for premenopausal women also include temporary suppression of ovarian oestrogen synthesis by luteinising hormone releasing hormone (LHRH) agonists, or permanent interruption through surgical removal (oophorectomy) or radiotherapy. The optimal duration of LHRH agonist therapy has not yet been defined, but usually this treatment is given for 2–5 years depending on tolerance and risk, concomitantly with tamoxifen. Aromatase inhibitors (AIs) are contraindicated in premenopausal women because they stimulate oestrogen production by the functioning ovaries. Their role in association with an LHRH agonist is currently being evaluated in clinical trials.
AIs are considered to be an important component of endocrine therapy for postmenopausal women. AIs decrease oestrogen production by inhibiting aromatase, an enzyme of the cytochrome P450 family, which converts androgens to oestrogen. In postmenopausal women, aromatase is the primary source of oestrogen synthesis and is present in peripheral tissues including fat, muscle, normal breast tissue, liver, and brain. It is also present in breast cancer tissue of endocrine-responsive disease. AIs are not able to overcome ovarian aromatase activity. Therefore, only postmenopausal women or women with non-functioning ovaries may benefit from therapy with AIs. Results from large randomised studies support the use of AIs for adjuvant therapy in postmenopausal women with hormone receptor-positive breast cancer.
AIs are beneficial when given at the beginning (ATAC, BIG 1-98), after 2–3 years of tamoxifen (IES, ABCSG-8, ARNO-95, ITA, BIG 1-98), or after 5 years of tamoxifen (NCIC–CTG MA.17). All studies have shown superiority of AI over tamoxifen in terms of disease-free survival (DFS) in the adjuvant setting [28–32]. Their benefit in terms of overall survival (OS) is still controversial and appears to be very limited (1–2% for upfront and sequential strategies respectively) [33]. Available guidelines support the use of AIs for most patients, unless contraindicated or badly tolerated [1, 8]. However, five years of tamoxifen alone is still a viable option for certain low-risk patient categories and when AIs are contraindicated or not well tolerated. Initial use of an AI is the preferred option in patients at higher risk of relapse (large tumour size, node positivity, HER2-positive disease) and has a good safety profile with the majority of the adverse events being mild. The large adjuvant trials report variable incidence of arthralgia and musculoskeletal complaints (5–38%) [28, 29]. However, several subsequent studies have shown that the rate of arthralgia seen in the community is significantly higher than initially reported in clinical trials, reaching about 30% and being an important cause of non-compliance with adjuvant HT.
As a consequence of oestrogen deprivation, patients on AI therapy often have a loss of bone density and an increased risk of fractures. Postmenopausal women with breast cancer are already at higher risk for the development of osteoporosis compared with the general population, and the use of drugs that can negatively affect bone mass in such individuals can further increase this risk. Women at risk are advised to have regular bone mineral density (BMD) measurements. The guidelines recommend that patients who have a T-score = -2.0, but no additional risk factors when AI therapy is initiated, are monitored every 1–2 years for changes in BMD and risk status [34]. Patients with a T-score < -2.0 at the initiation of AI treatment should receive a bisphosphonate. Vitamin D3 and calcium supplementation are also recommended for patients beginning AI therapy [34]. The other common side effects of AIs are vasomotor instability resulting in hot flushes, irritability and emotional problems, all very difficult to manage. One should be aware of the importance of quality of life and treatment side effects, particularly when patients are at low risk for disease recurrence. Compliance with endocrine therapy is challenging and has been shown to worsen with every additional year of prescribed therapy [35, 36].
More recently, studies have focused on the role of extended adjuvant HT either by prolonging the use of tamoxifen for 10 years or evaluating switching strategies using AIs after five years of tamoxifen [37–40]. Tamoxifen given for a period longer than five years has shown a slight superiority but was also associated to more side effects, particularly endometrial. This approach is reserved for certain high risk women still premenopausal after five years of tamoxifen. For postmenopausal women, AIs are a better option as extended adjuvant HT. The most commonly prescribed adjuvant endocrine therapies are shown in Table 4.
Adjuvant anti-HER2 therapy
HER2 is a member of the ErbB protein family, more commonly known as the epidermal growth factor receptor family. HER2 is a trans-membrane oncoprotein, found in high levels in 20–25% of all breast cancers. Tumours that overproduce HER2 tend to be more aggressive and more likely to recur than those that do not. HER2 overexpression/amplification is a marker of worse prognosis (associated with shorter DFS and OS) and a predictive marker for efficacy of anti-HER2 therapies such as the monoclonal antibody trastuzumab and the small HER1/HER2 tyrosine kinase inhibitor lapatinib. Patients with early HER2-positive breast cancer should be treated with anti-HER2 targeted therapy. The only agent approved so far for use in the adjuvant setting is trastuzumab.
Consistent benefits (39–52% of reduction of recurrence rate and a 30% reduction in mortality) have been reported with chemotherapy and trastuzumab compared with chemotherapy alone, across all pivotal adjuvant trastuzumab studies [41, 42]. Some questions related to trastuzumab use in the adjuvant setting still remain unanswered, such as the optimal timing, optimal duration, optimal chemotherapy regimens and its role in small node-negative tumours. The empirical standard for trastuzumab is one year, although there is some evidence, particularly in the FinHer study that a shorter duration of treatment is also effective and both economically attractive and potentially less toxic [43]. Ongoing trials are evaluating other treatment durations, e.g. 2 years, 6 months and 3 months. Trastuzumab is associated with the development of congestive heart failure (usually reversible) in the range of 0.5% to 3.9%, especially in patients at risk (advanced age, obesity, arterial hypertension, lower normal range of left ventricular ejection fraction (LVEF) at the start of treatment and prior therapy with anthracyclines). For this reason cardiac function should be carefully monitored before and during the treatment with trastuzumab and trastuzumab should be avoided if the LVEF < 50% [1]. Lapatinib is an orally available HER1– and HER2-targeted tyrosine kinase inhibitor, approved for the treatment of women with HER2-positive, pretreated, metastatic breast cancer and currently being evaluated in the (neo) adjuvant settings.
Conclusion
Traditional clinical predictors of response to therapy often fail to accurately predict which patients will experience metastasis. Prognostic gene signatures can differentiate subpopulations based on risk of relapse and there is a suggestion that these signatures may be most useful in identifying the low-risk patients who can safely be spared from adjuvant chemotherapy. Predictive gene signatures have the potential to aid the decision of which therapy to use in each patient in order to maximise individual benefit and minimise individual toxicity, although advances in this latter area have so far been less successful. Given the emerging understanding of breast cancer as a group of biologically distinct diseases, it is likely that the most promising approaches will involve personalised medicine with targeting of a particular weakness of an individual or group of related tumours rather than general cytotoxic approaches. Attempts at genetic modification and vaccine strategies have been promising in preclinical trials and may prove fruitful in future clinical trials.
Author for correspondence
Professor Fatima Cardoso, MD
Head, Breast Cancer Unit and Breast Cancer Research Director
Champalimaud Cancer Center
Av De Brasília – Doca de Pedrouços
PT-1400-048 Lisbon, Portugal
Co-authors
Ivana Bozovic-Spasojevic, MSc, MD
Clinical and Translational Research Fellow
Breast International Group
Otto Metzger Filho, MD
Research Fellow
Jules Bordet Institute
7/F, 121 Boulevard de Waterloo
BE-1000 Brussels, Belgium
References
1. Kataja V, Castiglione M. Primary breast cancer: ESMO clinical recommendation for diagnosis, treatment and follow-up. Ann Oncol. 2009;(Suppl 4):iv10-iv14.
2. Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55:74-108.
3. Reis LAG, Melbert D, Krapcho M, et al., editors. SEER cancer statistic review; 1975-2004, National Cancer Institute. Bethesda, MD; 2007.
4. Key TJ, Verkasalo PK, Banks E. Epidemiology of breast cancer. Lancet Oncol. 2001;2:133-40.
5. Kellen E, Vansant G, Christiaens MR, et al. Lifestyle changes and breast cancer prognosis: a review. Breast Cancer Res Treat. 2009;114:13-22.
6. Ha M, Mabuchi K, Sigurdson AJ, et al. Smoking cigarettes before first childbirth and risk of breast cancer. Am J Epidemiol. 2007;166:55-61.
7. Haybittle JL, Blamey RW, Elston CW, et al. A prognostic index in primary breast cancer. Br J Cancer. 1982;45(3):361-6.
8. Goldhirsch A, Inge JN, Gelber RD, et al. Thresholds for therapies: highlights of the St Gallen International Expert Consensus on the primary therapy of early breast cancer. Ann Oncol. 2009;20(8):1319-29.
9. Olivotto IA, Bajdik CD, Ravdin PM, et al. Population-based validation of the prognostic model ADJUVANT! for early breast cancer. J Clin Oncol. 2005;23:2716-25.
10. van’t Veer LJ, Dai H, van de Vijver MJ, et al. Gene expression profiling predicts clinical outcome of breast cancer. Nature. 2002;415(6871):530-6.
11. van de Vijver, He YD, van’t Veer LJ, et al. A gene-expression signature as a predictor of survival in breast cancer. N Eng J Med. 2002;347:1999-2009.
12. Paik S, Shak S, Tang G, et al. A multigene assay to predict recurrence of tamoxifen-treated, node-negative breast cancer. N Engl J Med. 2004 Dec 30;351(27):2817-26.
13. Mamounas EP, Tang G, Fisher B, et al. Association between the 21-gene recurrence score assay and risk of locoregional recurrence in node-negative, estrogen receptor-positive breast cancer: results from NSABP B-14 and NSABP B-20. J Clin Oncol; 2010 Apr;28(10):1677-83.
14. Bogaerts J, Cardoso F, Buyse M, et al. Gene signature evaluation as a prognostic tool: challenges in the design of the MINDACT trial. Nat Clin Pract Oncol. 2006;3(10):540-51.
15. Cardoso F, van’t Veer L, Rutgers E, Loi S, Mook S, Piccart-Gebhart MJ. Clinical application of the 70-gene profile: the MINDACT trial. J Clin Oncol. 2008 Feb;26(5):729-35.
16. Sparano JA. TAILORx: trial assigning individualized options for treatment (Rx). Clin Breast Cancer. 2006 Oct;7(4):347-50.
17. Perou CM, Sorlie T, Eisen MB, et al. Molecular portraits of human breast tumours. Nature. 2000 Aug; (6797):406:747-52.
18. Zhiyuan H, Cheng F, Charles P, et al. The molecular portraits of breast tumors are conserved across microarray platforms. BMC Genomics. 2006 Apr 27;7:96.
19. Azambuja E, Cardoso F, De Castro G, et al. Ki67 as prognostic marker in early breast cancer: a meta-analysis of published studies involving 12,155 patients. Br J Cancer. 2007 May; 96(10):1504-13.
20. Sotiriou S, Wirapati P, Loi S. et al. Gene expression profiling in breast cancer: understanding the molecular basis of histologic grade to improve prognosis. J. Natl Cancer Inst. 2006 Feb;98(4):262-72.
21. Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005 May; 365(9472):1687-717.
22. Nowak AK, Ferguson T, Wilcken NR, Ghersi D. A meta-analysis of taxanes in adjuvant chemotherapy (ACT) of early breast cancer (EBC) (Abstract 545). J Clin Oncol. 2007; 25:S18.
23. Ravdin PM, Burris HA, Cook G, et al. Phase II trial of docetaxel in advanced anthracycline-resistant or anthracenedione-resistant breast cancer. J Clin Oncol. 1995;13:2879-85.
24. Sparano JA, Wang M, Martino S, et al. Weekly paclitaxel in the adjuvant treatment of breast cancer. N Engl J Med. 2008;358:1663-71.
25. Shapiro CL, Recht A. Side effects of adjuvant treatment of breast cancer. N Engl J Med. 2001 Jun;344(26):1997-2008.
26. Love RR, Barden HS, Mazess RB, Epstein S, Chappell RJ. Effect of tamoxifen on lumbar spine bone mineral density in postmenopausal women after 5 years. Arch Intern Med. 1994;154:2585-8.
27. Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst. 1998;90:1371-88.
28. ATAC, Trialists’ Group. Effect of anastrozole and tamoxifen as adjuvant treatment for early-stage breast cancer: 100-month analysis of the ATAC trial. Lancet Oncol. 2008;9(1):45-53.
29. BIG 1-98 Collaborative Group. A comparison of letrozole and tamoxifen in postmenopausal women with early breast cancer. N Engl J Med. 2005;353:2747-57.
30. BIG 1-98 Collaborative Group. Letrozole therapy alone or in sequence with tamoxifen in women with breast cancer. N Engl J Med. 2009 Dec;361:766-76.
31. Coombes RC, Kilburn LS, Snowdon CF, et al. Survival and safety of exemestane versus tamoxifen after 2–3 years’ tamoxifen treatment (Intergroup Exemestane Study): a randomised controlled trial. Lancet. 2007 Feb; 369(9561):559-70.
32. Jakesz R, Jonat W, Gnant M, et al. Switching of postmenopausal women with endocrine-responsive early breast cancer to anastrozole after 2 years’ adjuvant tamoxifen: combined results of ABCSG trial 8 and ARNO-95 trial. Lancet. 2005;366:455-62.
33. Dowsett M, Cuzick J, Ingle J, et al. Meta-analysis of breast cancer outcomes in adjuvant trials of aromatase inhibitors versus tamoxifen. J Clin Oncol. 2010;28:509-18.
34. Hadji P, Aapro M, Brufsky A, et al. Practical guidance for the prevention of aromatase inhibitor-associated bone loss in women with breast cancer. Ann Oncol. 2008;19:1407-16.
35. Partridge AH, Wang PS, Winer EP, Avorn J. Nonadherence to adjuvant tamoxifen therapy in women with primary breast cancer. J Clin Oncol. 2003;21:602-6.
36. Partridge AH, LaFountain A, Mayer E, et al. Adherence to initial adjuvant anastrozole therapy among women with early-stage breast cancer. J Clin Oncol. 2008;26:556-62.
37. Peto R, Davies C, and the ATLAS investigators. ATLAS (Adjuvant Tamoxifen, Longer Against Shorter): international randomized trial of 10 vs 5 years of adjuvant tamoxifen among 11,500 women: preliminary results. In: program and abstracts of the 30th Annual San Antonio Breast Cancer Symposium; 2007 December 13–16; San Antonio, Texas: Abstract 48.
38. Goss PE, Ingle JN, Martino S, et al. Randomized trial of letrozole following tamoxifen as extended adjuvant therapy in receptor-positive breast cancer: updated findings from NCIC CTG MA.17. J Natl Cancer Inst. 2005;97:1262-71.
39. Mamounas EP, Jeong JH, Wickerham DL, et al. Benefit from exemestane as extended adjuvant therapy after 5 years of adjuvant tamoxifen: intention-to treat analysis of the National Surgical Adjuvant Breast and Bowel Project B-33 trial. J Clin Oncol. 2008;26:1965-71.
40. Jakesz R, Greil R, Gnant M, et al. Extended adjuvant therapy with anastrozole among post-menopausal breast cancer patients: results from the randomized Austrian Breast and Colorectal Cancer Study Group Trial 6a. J Natl Cancer Inst. 2007;99:1845-53.
41. Piccart-Gebhart MJ, Procter M, Leyland-Jones B, et al. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N Engl J Med. 2005;353:1659-72.
42. Romond EH, Perez EA, Bryant J, et al. Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer. N Engl J Med. 2005;353:1673-84.
43. Joensuu H, Kellokumpu-Lehtinen PL, Bono P, et al. Adjuvant docetaxel or vinorelbine with or without trastuzumab for breast cancer. N Engl J Med. 2006;354:809-20.